Sarah Ferguson has been diagnosed with malignant melanoma following the removal of a cancerous mole during treatment for breast cancer.
The Duchess of York had several moles removed and analyzed while having reconstructive surgery following a mastectomy, her spokesman said.
The duchess “remains in good spirits”, despite it being “distressing” to have another cancer diagnosis.
Sarah Ferguson is the third royal to announce a medical procedure this week.
Her spokesperson said: “Her dermatologist asked that several moles were removed and analyzed at the same time as the duchess was undergoing reconstructive surgery following her mastectomy, and one of these has been identified as cancerous.
“She is undergoing further investigations to ensure that this has been caught in the early stages.
“The duchess wants to thank the entire medical team which has supported her, particularly her dermatologist whose vigilance ensured the illness was detected when it was.
The statement also thanked the private medical team that supported the royal during her treatment.”
According to sources close to the duchess, she is back in the UK after initially recuperating in Austria.
In 2023, Sarah Ferguson had a diagnosis of breast cancer, following a routine mammogram screening.
The 64-year-old duchess was very public about her treatment, urging other women to get checked and using her podcast to raise awareness about breast cancer, wanting it to be a positive message to save others.
She went on to have a single mastectomy at King Edward VII hospital in London, a private clinic used by senior royals.
And having not been invited to the Coronation in May, at Christmas Sarah Ferguson appeared at Sandringham, walking to church with the rest of the Royal Family for the first time more than 30 years.
Sarah Ferguson was married to the Duke of York, Prince Andrew, for 10 years before they divorced in 1996.
They continue to share a home at Royal Lodge – a property owned by the Crown Estate at Windsor Great Park.
They have two daughters – Princess Beatrice, 35, and Princess Eugenie, 33 – and three grandchildren.
Kensington Palace said the procedure was successful but that the Princess of Wales was not expected to resume royal duties for months, and would remain in hospital for up to two weeks.
The palace did not disclose further details about Catherine’s condition but said it was not cancer-related.
Shortly after that announcement, Buckingham Palace said King Charles would receive treatment for a benign prostate condition and would visit an undisclosed hospital in the coming days.
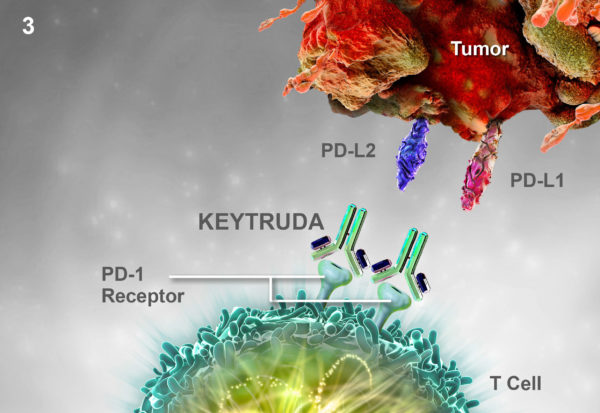
An immunotherapy drug can be
effective in some men with advanced prostate cancer, a major trial has shown.
The phase II clinical trial, led by the Institute of Cancer Research and the
Royal Marsden, involved 258 men with advanced prostate cancer who had run out
of all other options on treatment.
The men had stopped responding to
the main treatment options.
According to researchers, a small
proportion of men, described as “super responders”, remained well
even after the trial ended, despite a very poor prognosis before treatment.
Last week it was reported the same drug
had proved effective in treating advanced head and neck cancers.
Immunotherapy uses our own immune
systems to recognize and attack cancer cells.
The therapy is already being used as
a standard treatment for some cancers such as melanomas – and being tested on
many others too.
The study found that one in 20 men with advanced prostate cancer responded
to the drug pembrolizumab – and saw their tumors actually shrink or disappear
altogether.
The study, published in the Journal of
Clinical Oncology found that although a relatively small number, some of
the men gained years of extra life.
A further 19% saw some evidence of improvement.
Most patients in the study lived for an average of eight months on the drug.
The most dramatic responses were seen in patients whose tumors had mutations
in genes involved in repairing DNA.
Researchers are now investigating whether this group might benefit the most
from immunotherapy in a larger trial.
But first, a test to pick out who will respond best is needed, so that
doctors know which patients to give it to.
The number of people diagnosed with prostate cancer has been rising over the
last 10 years.
This is probably because the population is getting older and more people are
having PSA tests.
Around 30% of men with advanced or stage four prostate cancer survive their
cancer for five years or more after diagnosis.
Last week, a separate trial found the same drug kept some people’s advanced
head and neck cancers at bay for an average of two years – five times longer
than under chemotherapy.
Both studies are part of a growing body of research suggesting immunotherapy could offer hope to an increasing number of cancer patients.
Scientists from Massachusetts General Hospital have developed a drug that mimics sunlight to make the skin tan, with no damaging UV radiation involved.
According to researchers, the drug tricks the skin into producing the brown form of the pigment melanin in tests on skin samples and mice.
Evidence suggests the drug will work even on redheads, who normally just burn in the sun.
The team hopes the discovery could prevent skin cancer and even slow the appearance of ageing.
UV light makes the skin tan by causing damage.
Image source Pexels
This kicks off a chain of chemical reactions in the skin that ultimately leads to dark melanin – the body’s natural sun block – being made.
The drug is rubbed into the skin to skip the damage and kick-start the process of making melanin.
It is a markedly different approach to fake tan, which “paints” the skin without the protection from melanin, sun beds, which expose the skin to UV light or pills that claim to boost melanin production but still need UV light.
However, the team is not motivated by making a new cosmetic.
Tests, detailed in the journal Cell Reports, have shown the melanin produced by the drug was able to block harmful UV rays.
Eventually the scientists want to combine their drug with sun-cream to give maximum protection from solar radiation.
The way the drug works could also allow a ginger tan, as the genetic mutation that causes red hair and fair skin disrupts the normal process where UV light leads to dark melanin.
It is not yet clear if the drug might have the unintended consequence of affecting the glorious hair color, but it is thought the hair follicle is too deep in the skin for the drug to reach.
Anyway, whether you are ginger, blonde or brunette, the drug is not yet ready for commercial use.
A new study has shown that a fifth of people with advanced melanoma have no sign of tumors in their body after treatment with a pair of immunotherapy drugs.
The first survival data on using ipilimumab and nivolumab in combination showed 69% of patients, in a trial on 142, were still alive after two years.
Both drugs were developed by Bristol-Myers Squibb.
UK doctors leading the trial said the results were “very encouraging”.
More studies on the emerging field of immunotherapy will be presented later.
Photo Flickr
The immune system is a powerful defense against infection. However, there are many “brakes” built in to stop it attacking our own tissues.
Cancer – which is a corrupted version of healthy tissue – can take advantage of those brakes to evade assault.
Ipilimumab and nivolumab are designed to cut the brakes.
Both have become standard therapies in melanoma, but most researchers believe combination therapy will be essential.
The trial showed the survival rate after two years for ipilimumab alone was 53% and no patient’s tumors had completely disappeared.
The equivalent figures for combination therapy were 69% and 22%.
However, more than half of patients had severe to life-threatening side effects which stopped their treatment.
A much larger trial involving nearly 1,000 patients has already started releasing data, but has not run for long enough to produce survival figures.
According to a recent research, having more than 11 moles on the right arm indicates a higher-than-average risk of skin cancer or melanoma.
Counting moles on the right arm was found to be a good indicator of total moles on the body. More than 100 indicates five times the normal risk.
The study, published in the British Journal of Dermatology, used data from 3,000 twins in the UK.
Doctors could use the findings to identify those most at risk, it said.
Melanoma develops from abnormal moles, so the risk of being diagnosed with the disease is linked to the number of moles a patient has.
Researchers from King’s College London studied a large group of female twins over a period of 8 years, collecting information on skin type, freckles and moles on their bodies.
After repeating the exercise on a smaller group of around 400 men and women with melanoma, they came up with a quick and easy way to assess the risk of skin cancer.
Females with more than 7 moles on their right arm had nine times the risk of having more than 50 on their whole body.
Those with more than 11 on their right arm were more likely to have more than 100 on their body in total, meaning they were at a higher risk of developing a melanoma.
The findings could help doctors to identify those with an increased risk of developing a melanoma.
According to a new study, taller people have a slightly higher risk of breast cancer and skin cancer, among other cancers.
The Swedish study of five million people appears to support the theory that height and cancer risk are linked.
Its results found that for every extra 4in of height, when fully grown, the risk of developing cancer increased by 18% in women and 11% in men.
However, experts said the study did not take into account many risk factors and that tall people should not be worried.
They said that to reduce risk of cancer, the most important things to do are: giving up smoking, cutting down on alcohol, adopting a healthy diet and lifestyle.
Photo Getty Images
Previous studies have shown a link between height and an increased risk of developing cancer, although why it exists is not known.
In a preliminary report of the study, presented at the European Society for Paediatric Endocrinology conference, researchers from the Karolinska Institute in Stockholm describe how they tracked a large group of Swedish adults for more than 50 years.
Taller women had a 20% greater risk of developing breast cancer, they said, while taller men and women increased their risk of skin cancer (or melanoma) by 30%.
This study’s early findings are very similar in size to those found by other studies.
Dr. Emelie Benyi, who led the study, said the results could help to identify risk factors that could lead to the development of treatments.
She added: “As the cause of cancer is multi-factorial, it is difficult to predict what impact our results have on cancer risk at the individual level.”
Although it is clear that adult height is not a cause of cancer, it is thought to be a marker for other factors related to childhood growth.
Scientists say taller people have more growth factors, which could encourage cancer development, they have more cells in their body because of their size, which increases the risk of one of them turning cancerous, and a higher food intake, which also makes them more at risk of cancer.
Researchers have found that a genetically-engineered version of the cold sore virus (herpes simplex virus) could treat skin cancer.
T-Vec, the modified herpes virus, is harmless to normal cells but when injected into tumors it replicates and releases substances to help fight the cancer.
The findings, published in the Journal of Clinical Oncology, show the therapy could lengthen survival by years – but only for some melanoma patients.
The treatment is not yet licensed.
Similar “immunotherapy” treatments for melanoma are already available in the US and in Europe, but researchers believe T-Vec would be a welcome addition to these.
It would also be the first melanoma treatment that uses a virus.
The latest study is the largest ever randomized trial of an anti-cancer virus and involved 436 patients from 64 centers in the US, the UK, Canada and South Africa who had inoperable malignant melanoma.
UK trial leader Prof Kevin Harrington, from the Institute of Cancer Research, London, said: “There is increasing excitement over the use of viral treatments like T-Vec for cancer, because they can launch a two-pronged attack on tumors – both killing cancer cells directly and marshalling the immune system against them.
“And because viral treatment can target cancer cells specifically, it tends to have fewer side effects than traditional chemotherapy or some of the other new immunotherapies.”
Although it has not yet been licensed, doctors are excited about the very real prospect of a brand new type of treatment for advanced melanoma – and, in the future, possibly other cancers too.
The idea of using viruses to enter and kill cancerous cells has been gathering scientific pace and kudos.
This latest study in the Journal of Clinical Oncology is the largest ever randomized trial of an anti-cancer virus and provides tantalizing evidence that the treatment concept could soon be moved into the clinic, after decades of work in the lab.
Researchers now want to do more studies to identify which patients might benefit from the treatment and whether it should be used alongside other melanoma drugs that are already approved.
Drug regulators will be watching closely and will soon make a final decision about T-Vec.
Damage to the skin by the sun’s harmful UV rays increases your risk of developing this cancer.
The US researchers have developed personalized cancer vaccines that target unique genetic errors in a patient’s tumor.
Safety tests on three people, published in the journal Science, showed the immune system could be trained to fight skin cancers.
The research team, mainly based in St Louis and Oklahoma City, says the early results mark a “significant step” towards personalized cancer vaccines.
UV light can transform healthy skin cells into deadly melanomas by damaging the DNA.
The tumors are a genetic mess, containing hundreds of random mutations that are different in every patient.
The mutations can change the proteins that stick out from the surface of cells and act like identifying flags.
The team analyzed the genetic mutations to predict the new and unique flags that would be flown by the cancer cells.
A computer algorithm then analyzed the new flags, known as neoantigens, to decide which would be the best targets for a vaccine.
Personalized vaccines were given to three patients with advanced tumors in 2013. All had already been treated with another therapy – ipilimumab.
One was in remission and has stayed cancer-free; another still has stable tumors; and the third patient’s tumor shrank in the months after the vaccine before returning to its original size and remaining stable.
The team is, at this stage, testing just the safety of the vaccine and whether it provokes an immune response.
They say it was successful on both counts.
One of the researchers, Dr. Gerald Linette, said: “Our team is very encouraged by the quality of the immune response directed against the melanoma neoantigens in all three patients.
“Our results are preliminary, but we think the vaccines have therapeutic potential.”
His colleague, Dr Beatriz Carreno, added: “These findings represent a significant step toward more personalized immunotherapies.”
The personalized vaccine approach has a number of hurdles to clear.
For a start, proper clinical trials are needed to prove that the immune boost actually makes a difference to controlling the tumor.
There are also questions about cost and the time it takes – currently three months – to develop each person’s vaccine.
However, if the approach proves successful it could be useful in other highly mutated cancers such as those found in the lung.
They may also have a role in breast and ovarian cancers in women with BRCA mutations, such as Angelina Jolie, which also tend to be very mutated.
Three Dog Night keyboardist and vocalist Jimmy Greenspoon died from metastatic melanoma on March 11 at the age of 67.
Jimmy Greenspoon formed the band in 1968 with Danny Hutton, Cory Wells, Chuck Negron, Joe Schermie, Mike Allsup and Floyd Sneed.
He was first diagnosed with the disease on October, 2014 after a tumor was removed from his brain, spots were also found on his right lung and on his liver.
Soon after his sad diagnosis Jimmy Greenspoon set up a GoFundMe page in hopes of donations to help with the high costs of his medical treatments and care revealing that he would be a cancer patient for the rest of his day and the costs would be very high.
On March 10, Jimmy Greenspoon’s wife Susie posted to the band’s Facebook page that Jimmy was nearing the end of his battle with cancer revealing that the past few days have been very difficult for Jimmy and the family revealing that they were keeping Jimmy as comfortable as possible.
Three Dog Night made the announcement of his death on Facebook.
“We are very saddened at the passing of our dear friend and longtime band mate, Jimmy Greenspoon. Jimmy died peacefully at home today surrounded by his family. Please keep him and his loved ones in your prayers and your hearts,” the statement read.
Jimmy Greenspoon’s vocals can be heard on Three Dog Night’s biggest hits including Joy to the World, Black and White, Never Been to Spain and Your Song.
He continued to tour with his band until he came down with his illness.
Jimmy Greenspoon also performed alongside legends including Eric Clapton, Jimi Hendrix and the Beach Boys.
James Rebhorn, known for his roles in TV series Homeland and Scent of a Woman movie, has died from skin cancer at the age of 65.
James Rebhorn died at his home in South Orange, New Jersey, his agent Dianne Busch said.
The actor’s career spanned five decades and saw him appear in TV shows including The Good Wife and 30 Rock and films such as Meet the Parents, My Cousin Vinny, Carlito’s Way and Basic Instinct.
Diagnosed with melanoma in 1992, James Rebhorn continued working until last month.
Diagnosed with melanoma in 1992, James Rebhorn continued working until last month
James Rebhorn’s agent told The Hollywood Reporter: “He fought it all this time.
“He died [on] Friday afternoon at his home in New Jersey, where he had been receiving hospice care for a week and a half.”
James Rebhorn had more than 100 screen credits, one of the most recent being for Homeland, in which he played Frank Mathison, the father of Claire Danes’ CIA officer Carrie Mathison.
His films included The Talented Mr. Ripley, in which he played a shipping magnate.
James Rebhorn is survived by his wife Rebecca Linn and two daughters.
Vinnie Jones revealed he has had several lumps removed after being diagnosed with skin cancer.
The 48-year-old actor and footballer noticed a small blemish below his eye in February, thinking it was “a blackhead or a wart”.
A check-up revealed it was melanoma, the most serious type of skin cancer, which kills 1,300 men and 900 women every year.
Doctors have since found more tumors, but Vinnie Jones told The Sun he would fight it with “everything I’ve got”.
“When the doctor said I had skin cancer, the first thing I thought was <<how long have I got?>>” Vinnie Jones told the newspaper.
“It’s weighing very heavily on me all the time,” he said.
Malignant Melanoma is largely preventable by avoiding strong sunlight and using high-factor sun creams.
Vinnie Jones revealed he has had several lumps removed after being diagnosed with skin cancer
Treatment is more likely to be successful if melanoma is spotted early.
Vinnie Jones said that, subsequent to the removal of the tumor under his eye, doctors had found more cancer in the same area and, two months ago, he had a third operation to remove a tumor from the back of his head.
He blamed his outdoor lifestyle for the cancer – noting that after growing up on the football pitch, he had moved to Los Angeles to pursue a film career.
Now working with the Melanoma Research Foundation, Vinnie Jones urged people to be more aware of exposure to the sun.
“Footballers never put on sunblock and they should all be wearing it,” he said.
“Kids should all be wearing it every time they play sport.”
“If you spot something on your skin that doesn’t feel right… get it checked out immediately.”
Vinnie Jones also revealed his wife Tanya had been fighting skin cancer, a result of drugs she had been taking since having a heart transplant 26 years ago.
The star, who has appeared in films including X-Men: The Last Stand and Lock,Stock and Two Smoking Barrels, was previously captain of the Welsh Football Team and played for Wimbledon, Chelsea and QPR, among others.
Vinnie Jones’ revelation comes days after fellow actor Hugh Jackman disclosed he had been treated for skin cancer.
Melanoma cells manage to stay alive during treatment with BRAF/MEK inhibitors by shifting how they produce energy, researchers have discovered.
Identifying the mechanism behind melanoma resistance to treatment suggests possible strategy for improvement.
A multi-institutional study has revealed that BRAF-positive metastatic malignant melanomas develop resistance to treatment with drugs targeting the BRAF/MEK growth pathway through a major change in metabolism. The findings, which will be published in Cancer Cell and have been released online, suggest a strategy to improve the effectiveness of currently available targeted therapies.
“We were surprised to find that melanoma cells treated with the BRAF inhibitor vemurafenib dramatically change the way they produce energy to stay alive,” says David E. Fisher, MD, PhD, chief of Dermatology at Massachusetts General Hospital (MGH) and a co-corresponding author of the Cancer Cell paper.
“While current BRAF inhibitor treatment is a major improvement – shrinking tumors in most patients and extending survival for several months – patients eventually relapse. So there is an ongoing need to improve both the magnitude and durability of these responses.”
In about half the cases of malignant melanoma – the most deadly form of skin cancer – tumor growth is driven by mutations in the BRAF gene. Research by investigators at the MGH Cancer Center and elsewhere has shown that treatment with drugs that block BRAF activity temporarily halts tumor growth. Combining a BRAF inhibitor with a drug that targets MEK, another protein in the same growth pathway, strengthens and extends the antitumor response. The current study was designed to investigate how BRAF inhibition changes metabolic activity within melanoma cells and to find other possible treatment targets.
Melanoma cells survive by switching to oxidative phosphorylation to supply the energy they need.
The most common way that cells convert glucose into energy is called oxidative phosphorylation and largely relies on the activity of the cellular structures called mitochondria. Many cancer cells use an alternative mechanism that produces the energy compound ATP without involving mitochondria. A series of experiments by the MGH team revealed that the elevated BRAF activity in BRAF-positive melanoma cells suppresses oxidative phosphorylation by reducing expression of a transcription factor called MITF. Suppressing production of MITF reduced levels of a protein called PGC1α that regulates the generation and function of mitochondria. But melanoma cells treated with a BRAF inhibitor showed elevated MITF activity, along with increased expression of oxidative phosphorylation genes and greater numbers of mitochondria. By switching to oxidative phosphorylation to supply the energy they need, the tumor cells increased their ability to survive in spite of BRAF inhibitor treatment.
“These findings suggest that combination treatment with mitochondrial inhibitors could improve the efficacy of BRAF inhibitors in malignant melanoma,” says Fisher, the Wigglesworth Professor of Dermatology at Harvard Medical School.
“Several small molecules that target mitochondrial metabolism have been identified by investigators here at the MGH and elsewhere, and laboratory investigations of specific combinations of BRAF inhibitors with mitochondrial antagonists are currently underway.”
Melanoma is one of the most aggressive cancers. Only one patient in ten survives after 5 years from diagnosis. It is less common than other skin cancers, but it is much more dangerous if it is not found early. It causes the 75% of deaths related to skin cancer. Treatment consists of surgical excision which is completed by radiotherapy, chemotherapy, immunotherapy.
British researchers have found that melanoma, a deadly form of skin cancer, is able to fend off the body’s immune system.
Analysis of tumor and blood samples shows that melanoma knocks out the body’s best immune defence.
A potential test could work out which patients are likely to respond to treatment, the Journal of Clinical Investigation reports.
Cancer Research UK said the body’s response was a “complex puzzle”.
Previous work from the team at King’s College London showed that while patients with melanoma produced antibodies that could attack tumor cells, the immune system often seemed powerless to stop the cancer progressing.
But in the latest research they discovered that the subtype of antibody attracted by the melanoma cells was the most ineffective at mounting the right sort of response.
In samples from 80 melanoma patients researchers say that the conditions created by the tumor attract IgG4 antibodies, which mount the weakest response and in turn interfere with any “strong” IgG1 antibodies that might be present.
By mimicking the conditions created by melanomas, they showed that in the presence of tumor cells, the immune system sent out IgG4 antibodies, but when faced with healthy cells it functioned as expected with IgG1 circulating.
They also confirmed that IgG4 was ineffective in launching an immune attack against cancer cells.
Melanoma, a deadly form of skin cancer, is able to fend off the body’s immune system
In additional tests in 33 patients, they found that those with higher levels of the weak antibody IgG4 had a less favorable prognosis compared with those with levels nearer to normal.
Study author Dr. Sophie Karagiannis said: “This work bears important implications for future therapies since not only are IgG4 antibodies ineffective in activating immune cells to kill tumors but they also work by blocking antibodies from killing tumor cells.”
She said not only was IgG4 stopping the patient’s more powerful antibodies from eradicating cancer, but it could also explain why some treatments based on boosting the immune response may be less effective in some patients.
Co-author Prof. Frank Nestle said more work was needed on developing IgG4 as a potential test to improve patient care by helping to identify patients most likely to respond to treatments.
“This study can also inform the rational design of novel strategies to counteract IgG4 actions,” he added.
Dr. Kat Arney, science communications manager at Cancer Research UK, said: “There’s a lot we don’t yet understand about how our immune system recognizes and responds to cancer, so we’re pleased to have supported this new research that’s helping to solve such a complex puzzle.
“This work is still at an early stage, but it’s a step towards developing more effective treatments for skin cancer and potentially other types of cancer in the future.”
Scientists from the University of Southern California say fasting for short periods may help to combat cancer and boost the effectiveness of treatments.
Their study found fasting slowed the growth and spread of tumors and cured some cancers when it was combined with chemotherapy.
It is hoped that the discovery will prompt the development of more effective treatment plans and further research is now under way.
The study, published in the journal Science Translational Medicine, found that tumor cells responded differently to the stress of fasting compared to normal cells.
Instead of entering a dormant state similar to hibernation, the cells kept growing and dividing, in the end destroying themselves.
Lead researcher Professor Valter Longo, from the University of Southern California said: “The cell is, in fact, committing cellular suicide.
“What we’re seeing is that the cancer cell tries to compensate for the lack of all these things missing in the blood after fasting. It may be trying to replace them, but it can’t.”
Prof. Valter Longo and his team looked at the impact fasting had on breast, urinary tract and ovarian cancers in mice.
Fasting without chemotherapy was shown to slow the growth of breast cancer, melanoma skin cancer, glioma brain cancer and neuroblastoma – a cancer that forms in the nerve tissue.
In every case, combining fasting with chemotherapy made the cancer treatment more effective.
Multiple cycles of fasting combined with chemotherapy cured 20% of those with a highly aggressive form of cancer while 40% with a limited spread of the same cancer were cured.
None of the mice survived if they were treated with chemotherapy alone.
Researchers are already investigating the effects of fasting on human patients, but only a clinical trial lasting several years will confirm if human cancer patients really can benefit from calorie restriction.
However, they highlight that fasting could be dangerous for patients who have already lost a lot of weight or are affected by other risk factors, such as diabetes.
Results of a preliminary clinical trial will be presented at an annual meeting of the American Society of Cancer Oncologists (ASCO) in Chicago this June.
Prof. Valter Longo points out that the study only tests if patients could tolerate short fasts of two days before and one day after chemotherapy.
“We don’t know whether in humans it’s effective,” he said.
“It should be off-limits to patients, but a patient should be able to go to their oncologist and say, <<what about fasting with chemotherapy?>> or without if chemotherapy was not recommended or considered.”
Previous research led by Prof. Valter Longo showed that fasting protected normal cells from the effects of chemotherapy but it did not look at cancer cells.
It is now though fasting may be one way to make tumor cells weaker and more vulnerable.
Prof. Valter Longo added: “A way to beat cancer cells may not be to try to find drugs that kill them specifically but to confuse them by generating extreme environments, such as fasting, that only normal cells can quickly respond to.”
Hepatic Chemosat Delivery System was used to treat the first patients at the European Institute of Oncology (Instituto Europeo di Oncologia – IEO), Milan, Italy, announced Delcath System.
Two patients with inoperable liver-dominant metastases from ocular melanoma and gastric cancer were treated with the Generation One version of Chemosat system, and there were no procedure-related complications.
“The Chemosat system represents an important advancement in treatment options for cancers in the liver, which have significantly poorer survival rates compared to cancers that have spread predominantly to other organs. We believe this technology will help fill an important gap in the treatment of multiple tumor types in the liver because of its demonstrated ability to deliver concentrated doses of chemotherapeutic agent directly to the liver while helping to minimize systemic exposure. We are pleased to be the first center in Europe to begin offering this treatment to patients and look forward to exploring its potential with Delcath,” said Dr. Alessandro Testori, surgical oncologist and director of the Division of Melanoma and Skin-Muscle Sarcoma at the IEO.
Chemosat is a medical device that delivers chemotherapeutic drug directly to the liver. Pictures shows liver metastasis from a carcinoid tumor.
Chemosat is a medical device that utilizes chemosaturation technology.
This procedure supplies high doses of chemotherapeutic drugs directly to the liver and minimize the exposure of other organs to the drug. It can be repeated since it is a minimally invasive procedure.
Chemosat received CE Mark in April 2011 as a Class III medical device with an indication for the percutaneous intra-arterial administration of a chemotherapeutic agent (melphalan hydrochloride) to the liver.
“Since obtaining our CE Mark, Delcath has been committed to supporting the technology in the substantial international liver cancer market. These cases represent the first uses of Chemosat outside of a clinical trial—an exciting milestone for Delcath. There is no greater endorsement for Chemosat than to have the first European patients treated at an organization as prestigious as the IEO. We are delighted that the procedures were successfully performed, and look forward to continued collaborative progress with the IEO and the opportunity to open additional Chemosat treatment centers across Europe,” said Eamonn P. Hobbs, president and CEO of Delcath.
The Generation Two version of Chemosat is under review for CE Mark approval by the Notified Body.
On February 15, 2012 the IEO and Delcath will host a joint-press conference, at the IEO, and an update on patient status will be presented.
The cases were treated as part of the initial launch and training agreement with the IEO.
Chemosat is an investigational product in the United States and is not approved by the U.S. Food and Drug Administration.
On January 30, Erivedge (vismodegib) was approved by the U.S. Food and Drug Administration to treat adult patients with basal cell carcinoma, the most frequent type of skin cancer.
Erivedge (vesmodegib) was approved by FDA to treat metastatic basal cell carcinoma.
Genentech (division of Roche) developed the drug in collaboration with Curis. Erivedge will available in pharmacies within one or two weeks. The capsules have to be taken once a day and its safety in children it is unknown.
Patients with locally advanced basal cell cancer who are not candidates for surgery or radiation and patients with metastasis (cancer spread to other parts of the body) may benefit from this medicine.
Erivedge is the first FDA-approved drug for metastatic basal cell carcinoma.
This drug was approved earlier under the FDA’s priority review program for drugs that may offer major advances in treatment.
Erivedge (Vismodegib) inhibits the Hedgehog pathway in the cancer cells.
This pathway is active in most basal cell cancers and only in a few normal tissues (hair follicles).
“Our understanding of molecular pathways involved in cancer, such as the Hedgehog pathway, has enabled the development of targeted drugs for specific diseases. This approach is becoming more common and will potentially allow cancer drugs to be developed more quickly. This is important for patients who will have access to more effective therapies with potentially fewer side effects,” said Richard Pazdur, M.D., director of the Office of Hematology and Oncology Products in the FDA’s Center for Drug Evaluation and Research.
A clinical study that enrolled 96 patients with locally advanced or metastatic basal cell carcinoma tested the safety and effectiveness of Erivedge.
Researchers recorded the percentage of patients who experienced complete or partial shrinkage or disappearance of the cancerous lesions. In 30% of the patients with metastatic disease a partial response was found and in 43% of the patients with locally advanced disease complete or partial responses were noted. The median progression-free survival rate for both groups was 9.5 months.
Basal cell carcinoma begins in the lower part of top layer of the skin (epidermis) on areas of skin that are exposed to ultraviolet radiation. It is mostly a slow growing and painless form of skin cancer. Most skin cancers appear in older people or in people with an weak immune systems. Every year around 1,000,000 of new cases of skin cancers (aside from melanoma) are diagnosed in U.S. and around 1,000 deaths are recorded.
Important Safety Information for Erivedge
“Erivedge can cause a baby to die before it is born (be stillborn) or cause a baby to have severe birth defects based on how the medicine interacts with the body.
• Female patients who can become pregnant should speak with their healthcare provider about the risks of Erivedge to their unborn child. Their healthcare provider should do a pregnancy test within seven days before they start taking Erivedge to find out if they are pregnant. Women should avoid pregnancy by using highly effective birth control before starting Erivedge, and continue during treatment and for seven months after their last dose. They should tell their healthcare provider right away if they have unprotected sex or think that their birth control has failed. Female patients must tell their healthcare provider right away if they become pregnant or think that they may be pregnant. Pregnant women are encouraged to participate in a program called the Erivedge pregnancy pharmacovigilance program by calling 1-888-835-2555.
• Male patients should always use a condom with a spermicide during sex with female partners while they are taking Erivedge and for two months after their last dose, even if they have had a vasectomy. Male patients should tell their healthcare provider right away if their female partner could be pregnant or thinks she is pregnant while they are taking Erivedge.
• Patients must not donate blood or blood products while they are taking Erivedge and for seven months after their last dose.
• The most common side effects of Erivedge are muscle spasms, hair loss, change in how things taste or loss of taste, weight loss, tiredness, nausea, diarrhea, decreased appetite, constipation, vomiting and joint aches. Another side effect may include missed monthly periods in females who can become pregnant.
• Patients should tell their healthcare provider if they have any side effect that bothers them or that does not go away.
• These are not all the possible side effects of Erivedge. For more information, please see the Full Prescribing Information for Erivedge, including the Boxed WARNING and Medication Guide.”
A team of researchers from University of Missouri Columbia has developed a method to detect melanoma cells when they start to spread into the blood stream and before they develop into tumors.
It is extremely important to identify the cell into the blood stream before they start to grow into a tumor. This may make the difference between curable an incurable melanoma.
Using photoacoustics, or laser-induced ultrasounds, cancer cells can be detected with higher efficiency than using current methods.
According to John Viator photoacoustics can identify metastasis before a tumor can be detected with MRIs or CT scans. The method is more sensitive and less expensive because the action can be performed on equipment that is more simplistic than the methods used to diagnose melanoma (MRIs or CT scans).
“Currently, metastatic disease, the phase of cancer where it is spreading throughout the body, is detected by performing body scans, looking for macroscopic tumors that are greater than a few millimeters in size. This method is a new paradigm where we detect cancer’s spread in the bloodstream by detecting single cells in blood samples. The ability to detect metastatic disease when it is still at the single cell level may allow treatment to be done in much lower doses, so that chemotherapy can be performed in such a way that is much easier on the patient,” said by John Viator, associate professor of biological engineering and associate professor of biomedical engineering and dermatology, who is leading the team.
Photoacoustics are being produced commercially for various cancer studies and clinical trials to receive the United States Food and Drug Administration’s approval.
Detecting melanoma cells when they start to spread into the blood stream, might be a way to improve treatment and prevention.
“We hope one day to use this method as a general screening tool for everyone, just like women have to get mammograms. After a certain age, it would be part of your routine physical. If you’re predisposed to metastatic melanoma and if the disease is ‘caught early’ by our detection system before the patient shows symptoms, then the chances of survival can be up to 90 percent,” said biological engineering graduate Ben Goldschmidt.
He has worked with the MU researchers team on designing a disposable flow cell for a melanoma detection system to make the device to be used commercially.
Melanoma is a malignant tumor developed from cells that produce the dark pigment (melanin), called melanocytes.
Melanin induces the color of the skin. Melanocytes are found mostly in skin, but they are also presents in other parts of the body, including the bowel and the eye (uveal melanoma). Melanoma can develop in any part of the body that contains melanocytes.
Melanoma is occurs less frequent than other skin cancer, but is more severe and causes the most of the deaths from skin cancer. The disease can start from a mole that is scratched very often, or cut or too exposed to the ultraviolet radiation. Melanoma can become metastatic and spread rapidly into other organs, and the treatment is difficult.
This year around 76,250 new cases of melanoma will be diagnosed and about 9,180 from this cancer will occur, according to the estimations made by the National Cancer Institute.
The multi-vitamin pills are taken daily by millions of people in the world, hoping to ward off ill-health.
However, a major study showed that the vitamin pills do nothing for our health.
A team of French researchers spent more than 6 years following 8,000 people and found that those taking supplements were just as likely to have developed cancer or heart disease as those who took an identical-looking dummy pill.
And when they were questioned on how healthy they felt, there was hardly any difference between the two groups.
Experts said the study – one of the most extensive carried out into vitamin pills – suggested that millions of consumers may be wasting their money on supplements.
Many users fall into the category of the “worried well” – healthy adults who believe the pills will insure them against deadly illnesses – according to Catherine Collins, chief dietician at St. George’s Hospital in London.
Catherine Collins said: “It’s the worried well who are taking these pills to try and protect themselves against Alzheimer’s disease, heart attacks and strokes.
“But they are wasting their money. This was a large study following people up for a long period of time assessing everything from their mobility and blood pressure to whether they were happy or felt pain.”
A team of French researchers spent more than 6 years following 8,000 people and found that those taking supplements were just as likely to have developed cancer or heart disease as those who took an identical-looking dummy pill
Multi-vitamin supplements have become increasingly popular as a quick and easy way of topping up the body’s nutrient levels.
But a series of studies have indicated that, for some people, they could actually be harmful.
Two studies published in 2010 suggested supplements could raise the risk of cancer.
One found pills containing vitamin E, ascorbic acid, beta-carotene, selenium and zinc increased the risk of malignant melanoma, the deadliest form of skin cancer, four-fold.
Other study discovered women on a daily multi-vitamin pill increased their risk of breast cancer by up to 20%.
While the evidence that vitamins can do harm is still limited, the latest study seems to confirm that many people are at the very least taking them unnecessarily.
The team of French researchers, led by experts at Nancy University, tracked 8,112 volunteers who took either a placebo capsule, or one containing vitamin C, vitamin E, beta-carotene, selenium and zinc, every day for just over six years.
They assessed the state of their health at the beginning and end of the trial, taking a quality of life survey designed to measure everything from mobility and pain to vitality and mental health.
When researchers analyzed how many in each group had gone on to develop serious illnesses over the years, they found little difference.
In the supplement group, 30.5% of patients had suffered a major health “event”, such as cancer or heart disease. In the placebo group, the rate was 30.4%.
There were 120 cases of cancer in those taking vitamins, compared to 139 in the placebo group, and 65 heart disease cases, against 57 among the dummy pill users.
In a report on their findings, published in the International Journal of Epidemiology, the researchers said: “The perception that supplementation improves general well-being is not supported by this trial.”
Catherine Collins said the results of the study “reinforce the idea that if you’re worried about your health and start taking multi-vitamins, you will still be worried about it six years later”.
The Health Supplements Information Service, which is funded by supplements manufacturers, said the finding that vitamins had no impact on how people perceived their health was “to be expected”.
Spokeswoman Dr. Carrie Ruxton said: “The role of vitamin supplements is to prevent deficiencies and make sure people are receiving their recommended levels.
“They won’t have a measurable impact on how you feel on a day-to-day basis but what they are doing is topping up your recommended levels to the right amount. They are not meant to be a magic bullet.”
A study published in the American Journal of Clinical Nutrition showed that moderate consumption of wine can increase bone mineral density (BMD) and prevent post-menopausal fractures linked to osteoporosis.
Researchers from the University of East Anglia and Kings College London have studied over 1,000 pairs of female of age about 55. The subjects were questioned about their dietary habits and the scientists have measured the thickness of their bones in the hip joint, the spine and the top of the femur. These are the places in which the bones are broken more often when osteoporosis occurred in post-menopause.
Moderate wine drinkers had higher bone density in the spine and the hip than non-drinkers, or drinkers of other types of alcohol (spirit, beer).
A glass of wine a day could prevent osteoporosis, Alzheimer's, stroke and heart attack, but excessive drinking increases risks of these conditions.
A diet of fish and chips, baked beans, meat pies and cooked meats apparently lowered bone mineral density and a diet high in fruit and vegetables seemed to have no substantial benefits.
“Moderate intakes of alcohol from wine were associated with a higher bone mineral density and the consumption of a traditional 20th-century English diet was linked with a lower bone density,” said scientists.
The findings come before World Osteoporosis Day on October 20, 2011.
Polyphenols, found in the skin of grapes, could help the bones strengthening, not the alcohol, other studies have suggested. Polyphenols are known as antioxidants and they help to prevent heart and brain diseases (stroke, Alzheimer’s), besides osteoporosis.
While a glass a day could prevent osteoporisis, and smaller studies have suggested alcohol might have a protective effect, heavy drinking is known as a major factor that weakens the bones, and leads to osteoporosis.
It is not the first time when researchers focus on the linkage between osteoporosis and wine.
Katherine Tucker, professor of nutrition and epidemiology at the USDA Human Nutrition Research Center at Tufts University in Boston, said in 2004 that beer could prevent osteoporosis in men bones, while wine is good for women bones. Beer contains silicon and wine polyphenols. The study was performed on 2,900 men and women, but there were not enough men who had drunk wine, nor women who had drunk beer, thus, the study only linked men to beer and women to wine. However, Professor Tucker said it is possible that men could benefit from two glasses of wine, while women from two cans of beer.
The study was presented at the American Society for Bone and Mineral Research annual meeting. Men who drank one to two beers a day had around 7% higher hip bone mineral density than nondrinkers. In women, increase was slightly less but was still significantly better than bone mineral density in nondrinkers.
The same message about the importance of moderation was sent at that time too, because “while two cans of beer or two 6 ounce [177,44 ml] glasses of wine are good for bones, drinking more is harmful,” and about distilled beverages (vodka or Scotch) “daily consumption of more than two drinks promotes osteoporosis,” Professor Tucker said.
What is osteoporosis?
In children bones grow and regenerate rapidly, but in adults the process is slower. Over the age of 30 a person starts to lose bone mineral density. Through life old bone is being destroyed by osteoclasts and new bone is formed by osteoblasts. The osteoblasts (cells that produce new bone) became gradually outnumbered by osteoclasts (cells that remove the calcium and phosphorous from an old bone). The balance between these two types of cells is very important for a healthy bone.
Osteoporosis occurs when bone mineral density is lower. The bones are fragile and break (fracture) easily.
Osteoporosis (porous bones, from Greek: ὀστέον/osteon meaning bone and πόρος/poros meaning pore) is a condition that causes bones to become weak and fragile and to break (fracture) easily. It appears frequently in the spine, wrist and hips. Osteoporosis is called a silent disease because lots of people become aware of it only until a fracture occurs.
The gold standard for diagnosis is dual energy X-ray absorptiometry (DXA, formerly DEXA). It measures bone mineral density and expressed it in standard deviations from a young adult reference population (T-score).
* T-score -1.0 or greater is normal
* T-score between -1.0 and -2.5 is low bone mass (osteopenia)
* T-score -2.5 or below is osteoporosis
Osteoporosis affects an estimated 75 million people in Europe, USA and Japan.
Steroid drugs, smoke, heavy drinking and a family history of osteoporosis are important risk factors.
Worldwide, an osteoporotic fracture is estimated to occur every 3 seconds, a vertebral fracture every 22 seconds.
Osteoporosis is estimated to affect 200 million women worldwide – approximately one-tenth of women aged 60, one-fifth of women aged 70, two-fifths of women aged 80 and two-thirds of women aged 90.
About 20-25% of hip fractures occur in men. The overall mortality is about 20% in the first 12 months after hip fracture and is higher in men than women.
It is estimated that the lifetime risk of experiencing an osteoporotic fracture in men over the age of 50 is 30%, similar to the lifetime risk of developing prostate cancer. (Source: International Osteoporosis Foundation).
Can osteoporosis be prevented?
First the risk factors have to be removed. Adequate nutrition (with food rich in proteins, calcium and vitamin D), daily moderate sun exposure (to stimulate vitamin D production) and adequate exercise can slow osteoporosis progression and prevent fractures. An excessive exposure to ultraviolet radiation increases the risk of skin tumors or melanoma. Childhood and adolescence are the perfect times to improve bone mineral density through exercise and to prevent osteoporosis.
Taking a new step on preventing melanoma, Edmund G. Brown, Jr., California Governor, signed on October 9 SB 746 into a law that restricts persons under age of 18 from using indoor tanning devices.
The law takes effect starting January 1, 2012.
It is the first time in the U.S. when a state interdicts tanning beds use to minors. Senate Bill 746 replaces the current law, which allows teens (14-17 years old) to use tanning beds if they have parental permission.
Minimum 32 states regulate the use of tanning devices by teens. In 2010 Howard County, Maryland was the first jurisdiction that restricted tanning booths for children under 18. Texas has prohibited the use of tanning booths for persons under 16.
Senator Ted W. Lieu is the author of the bill in the Senate and the law was sponsored by AIM at Melanoma and the California Society of Dermatology & Dermatological Surgery (CalDerm) and backed by medical organizations and health insurers.
Illinois, New York, Ohio and Rhode Island have considered the same age limit for tanning beds prohibition, but they have to enact the law.
Indoor Tanning Association said the interdiction affects businesses, lots of them owned by women, as around 5 percent to 10 percent of its members’ customers are under 18.
Tanning salons are regulated by the state Department of Consumer Affairs and the federal Food and Drug Administration, said the organization.
Using a tanning device before the age of 20 increases the risk of melanoma by two times.
The linkage between tanning devices and melanoma was emphasized during the recent years.
Ultraviolet (UV) radiation from the sun and artificial sources (tanning beds and sun lamps) is a carcinogen, stated The United States Department of Health and Human Services in 2002.
“People under the age of 35 who are exposed to indoor tanning have a 75 percent increased risk of skin cancer, and the younger you are exposed to indoor tanning, the greater your risk of getting potentially fatal melanoma,” Dr. Peter Beilenson said in 2009, citing a study from the World Health Organization.
“Teenagers are much more likely to burn with indoor tanning. Fifty-eight percent report burning in indoor tanning. And burns, particularly at a young age, are clearly correlated with developing melanoma and other skin cancers later in life,” he said.
Repeated exposure to UV radiation from tanning devices before age of 35 is associated with a 75 percent increased risk of melanoma, and non-melanoma skin cancer (squamous cell carcinoma and basal cell carcinoma), studies show.
Exposure to UV can cause skin damage which is cumulative and can lead to skin cancers, or melanoma.
Around 30 million people in the U. S., including 2.3 million teens, use tanning beds annually.
The use of tanning devices before the age of 20 double the risk of developing melanoma. In women between the ages of 25 and 30 melanoma causes more deaths than all other cancers, while in women 30-34 this deadliest skin cancer comes second after the breast cancer.
“If everyone knew the true dangers of tanning beds, they’d be shocked. Skin cancer is a rising epidemic and the leading cause of cancer death for women between 25 and 29,” said Ted Lieu and cited a recent Stanford Cancer Institute study according to higher melanoma rates were found among girls and young women in areas of higher income.
“Indoor tanning is especially harmful because of the intense and dangerous type of UV rays emitted from the tanning beds. Moreover the skin damage is cumulative, so the more exposure one gets younger in life, the worse the harmful effects will be,” he said.
More than 3.5 million skin cancers in more than 2 million people are diagnosed annually. One in five Americans will develop skin cancer during the lifetime, it is estimated.
Jerry Brown was praised by the melanoma prevention supporters.
“California is expected to have 8,250 new cases of melanoma in 2011, or approximately 12 percent of the estimated 70,000 cases nationwide. Melanoma incidence rates have been increasing for the last 30 years, but have been growing most rapidly — three percent per year — since 1992 among young women ages 15 to 39. We encourage other states to follow California’s lead and help slow the incidence of potentially deadly skin cancer by prohibiting the use of commercial tanning devices by minors,” said dermatologist Ann F. Haas, MD, FAAD, former president of the CalDerm.
“I praise Governor Brown for his courage in taking this much-needed step to protect some of California’s most vulnerable residents – our kids – from what the ‘House of Medicine’ has conclusively shown is lethally dangerous: ultraviolet-emitting radiation from tanning beds,” said Ted Lieu.
“Girls in affluent California communities especially are surrounded by the message that being tanned all year round is cool. Pop music star Katy Perry is even singing about it,” said Christina Clarke of the Cancer Prevention Institute of California.
“The California Society of Dermatology and Dermatologic Surgery (CalDerm) and AIM at Melanoma Foundation, the bill’s two co-sponsors, applaud Governor Brown for taking the time to thoroughly understand the importance of this first-in-the-nation legislation. We also commend Senator Ted Lieu, his staff and the members of the California legislature who supported efforts to protect young Californians from the dangers of indoor tanning,” said Alex Miller, MD, President of CalDerm.
“This is a major victory in the fight against melanoma. It is alarming that so many young women are unnecessarily developing melanoma because of a recreational activity. We applaud Governor Brown for taking advantage of this unique opportunity to blaze a trail by banning minors from using tanning beds. We thank him for joining our fight against this preventable killer,” said Valerie Guild, president and founder of AIM at Melanoma.
Valerie Guild lost her daughter (age 26) because of melanoma. AIM at Melanoma was founded in memory of Charlie Guild and Jim Schlipmann (who died of melanoma at 44). It is the largest international melanoma foundation focused on melanoma research, patient advocacy, legislation, education and awareness. The foundation supports melanoma research efforts by hosting international research forums and is helping to create the first melanoma tissue bank, widely believed by the oncology community to be a key to major breakthroughs in melanoma research.
For more information on melanoma please visit www.AIMatMelanoma.org, www.aad.org, or contact the Academy at 1 (888) 462-DERM (3376).
Abraxane plus gemcitabine achieved a median overall survival of 12.2 months in patients with advanced pancreatic cancer, study reports. Patients with high-SPARC biomarker achieved significantly higher overall survival.
Celgene International Sàrl announced on October 6 that results from a clinical study of Abraxane (paclitaxel albumin-bound particles for injectable suspension) in combination with gemcitabine in 67 patients with previously untreated advanced pancreatic cancer were published in an online article by the Journal of Clinical Oncology.
Abraxane, approved by FDA for breast cancer, could be a life-prolonging drug for patients with advanced pancreatic cancer.
After the first phase of the study, the recommended Phase II dose was 125 mg/m2 of Abraxane followed by 1000 mg/m2 of gemcitabine on days 1, 8 and 15 of every 28-day cycle.
In Phase II, almost half of the patients responded (overall response rate was 48% (21/44)) and two-thirds experienced disease control (disease control rate was 68% (30/44)). The median progression-free survival was 7.9 months (95% CI: 5.8, 11.0) and the median overall survival (OS) was 12.2 months (95% CI: 8.9, 17.9). The one-year survival rate for patients was 48%.
Levels of secreted protein acidic and rich in crysteine (SPARC) were evaluated in 36 patients. These patients were classified as either high-SPARC (average z-score greater-than or equal to 0, n=19) or low-SPARC (average z-score <0, n=17). According to the study, a significant increase in OS was observed for patients in the high-SPARC group versus the low-SPARC group (median 17.8 vs. 8.1 months, p=0.0431). SPARC level remained a significant predictor of OS in a multivariate Cox regression model after adjusting for multiple clinical covariates including gender, race, age, treatment and baseline CA19-9 level (p=0.041). Of note, SPARC in the stroma correlated highly with OS (p=0.013), while SPARC in the tumor cells did not (p=0.15). This is particularly intriguing as SPARC expression in the stroma, but not in the tumor, has been associated with poor survival, suggesting that a unique mechanism of action of Abraxane may play a role in this reverse outcome.
Secreted protein acidic, rich in cysteine (SPARC) is an acidic, secreted extracellular matrix glycoprotein that plays a vital role in bone mineralization, cell-matrix interactions, and collagen binding. SPARC also increases the production and activity of matrix metalloproteinases, a function important to invading cancer cells within bone. Additional functions of SPARC beneficial to tumor cells include angiogenesis, proliferation and migration. Overexpression of SPARC is reported in many human cancers such as breast, prostate and colon.
The most common DLTs in the first phase of the study were sepsis and neutropenia. During the second phase, the most common grade 3 or higher Abraxane-related non-hematologic adverse events were fatigue (21%) and sensory neuropathy (15%). The most common grade 3 or higher treatment-related hematologic adverse events were neutropenia (67%), leukopenia (44%) and thrombocytopenia (23%).
These data are being confirmed in an ongoing, international, randomized phase III trial of Abraxane + gemcitabine vs. gemcitabine for patients with metastatic pancreatic cancer. Additional information about the trial can be found at: http://www.clinicaltrial.gov/ct2/show/study/NCT00844649?term=abraxane&cond=pancreatic%2Bcancer&phase=2&rank=2&show_locs=Y#locn.
These data are reported from an investigational study. Abraxane is not approved as a treatment for previously untreated advanced pancreatic cancer.
Pancreatic cancer is a malignant neoplasm of the pancreas. In typical usage, the term pancreatic cancer refers specifically to the significantly most common type of cancer, adenocarcinoma (and some variants thereof), that arises within the exocrine component of the pancreas, although the term can also reasonably be used to encompass less common types of cancer that also originate within the pancreas, and is quite frequently inclusive of the other exocrine cancers. Pancreatic cancer is the fourth most common cause of cancer death both in the United States and internationally.
Celgene International Sàrl, located in Boudry, in the Canton of Neuchâtel, Switzerland, is a wholly owned subsidiary and international headquarters of Celgene Corporation. Celgene Corporation, headquartered in Summit, New Jersey, is an integrated global pharmaceutical company engaged primarily in the discovery, development and commercialization of innovative therapies for the treatment of cancer and inflammatory diseases through gene and protein regulation. For more information, please visit the Company’s website at http://www.celgene.com.
Abraxane is a solvent-free chemotherapy treatment option for metastatic breast cancer which was developed using Celgene’s proprietary nab® technology platform.
This protein-bound chemotherapy agent combines paclitaxel with albumin, a naturally-occurring human protein. Abraxane is currently in various stages of investigation for the treatment of the following cancers: expanded applications for metastatic breast, non-small cell lung, malignant melanoma, pancreatic and gastric.
In 1967 Monroe E. Wall and Mansukh C. Wani isolated a mitotic inhibitor from the bark of the Pacific yew tree, Taxus brevifolia and named it taxol. Later named paclitaxel, the natural product has antitumor activity and is the active agent in Abraxane.
The U.S. Food and Drug Administration approved Abraxane for Injectable Suspension (paclitaxel protein-bound particles for injectable suspension) in January 2005 for the treatment of breast cancer after failure of combination chemotherapy for metastatic disease or relapse within six months of adjuvant chemotherapy. Prior therapy should have included an anthracycline unless clinically contraindicated. For the full prescribing information for Abraxane please visit http://www.abraxane.com.
Abraxane® for Injectable Suspension (paclitaxel protein-bound particles for injectable suspension) is indicated for the treatment of breast cancer after failure of combination chemotherapy for metastatic disease or relapse within 6 months of adjuvant chemotherapy. Prior therapy should have included an anthracycline unless clinically contraindicated.
ADVERSE EVENTS
Severe cardiovascular events possibly related to single-agent ABRAXANE occurred in approximately 3% of patients in the randomized trial. These events included chest pain, cardiac arrest, supraventricular tachycardia, edema, thrombosis, pulmonary thromboembolism, pulmonary emboli, and hypertension. Cases of cerebrovascular attacks (strokes) and transient ischemic attacks have been reported rarely. During postmarketing surveillance, rare reports of congestive heart failure and left ventricular dysfunction were observed, primarily among individuals with underlying cardiac history or prior exposure to cardiotoxic drugs.
In the randomized metastatic breast cancer study, the most important adverse events included alopecia (90%), neutropenia (all cases 80%; severe 9%), sensory neuropathy (any symptoms 71%; severe 10%), asthenia (any 47%; severe 8%), myalgia/arthralgia (any 44%; severe 8%), anemia (all 33%; severe 1%), nausea (any 30%; severe 3%), diarrhea (any 27%; severe <1%) infections (24%), vomiting (any 18%; severe 4%), and mucositis (any 7%; severe <1%).
Other adverse reactions have included ocular/visual disturbances (any 13%; severe 1%), renal dysfunction (any 11%; severe 1%), fluid retention (any 10%; severe 0%), hepatic dysfunction (elevations in bilirubin 7%, alkaline phosphatase 36%, AST [SGOT] 39%), hypersensitivity reactions (any 4%; severe 0%), cardiovascular reactions (severe 3%), thrombocytopenia (any 2%; severe <1%), and injection site reactions (<1%). In clinical trials and during postmarketing surveillance, dehydration was common and pyrexia was very common. Rare occurrences of severe hypersensitivity reactions have also been reported during postmarketing surveillance.
Please see full Prescribing Information, including Boxed WARNINGS, CONTRAINDICATIONS, WARNINGS AND PRECAUTIONS, and ADVERSE REACTIONS.
Important Safety Information
Abraxane for Injectable Suspension (paclitaxel protein-bound particles for injectable suspension) should be administered under the supervision of a physician experienced in the use of cancer chemotherapeutic agents. Appropriate management of complications is possible only when adequate diagnostic and treatment facilities are readily available.
Abraxane therapy should not be administered to patients with metastatic breast cancer who have baseline neutrophil counts of less than 1,500 cells/mm3. In order to monitor the occurrence of bone marrow suppression, primarily neutropenia, which may be severe and result in infection, it is recommended that frequent peripheral blood cell counts be performed on all patients receiving Abraxane.
Note: An albumin form of paclitaxel may substantially affect a drug’s functional properties relative to those of drug in solution. DO NOT SUBSTITUTE FOR OR WITH OTHER PACLITAXEL FORMULATIONS.
ADDITIONAL WARNINGS
The use of Abraxane has not been studied in patients with renal dysfunction. In the randomized controlled trial, patients were excluded for baseline serum bilirubin >1.5 mg/dL or baseline serum creatinine >2 mg/dL.
Pregnancy-Teratogenic Effects: Pregnancy Category D Abraxane can cause fetal harm when administered to a pregnant woman. If this drug is used during pregnancy, or if the patient becomes pregnant while receiving this drug, the patient should be apprised of the potential hazard to the fetus. Women of childbearing potential should be advised to avoid becoming pregnant while receiving treatment with Abraxane. Men should be advised to not father a child while receiving treatment with Abraxane.
Abraxane contains albumin (human), a derivative of human blood.
PRECAUTIONS
No drug interaction studies have been conducted with Abraxane. Caution should be exercised when administering Abraxane concomitantly with medicines known to inhibit or induce either CYP2C8 or CYP3A4.
Abraxane therapy should not be administered to patients with baseline neutrophil counts of less than 1,500 cells/mm3. It is recommended that frequent peripheral blood cell counts be performed on all patients receiving Abraxane. Patients should not be retreated with subsequent cycles of Abraxane until neutrophils recover to a level >1,500 cells/mm3 and platelets recover to >100,000 cells/mm3. In the case of severe neutropenia (<500 cells/mm3 for 7 days or more), during a course of Abraxane therapy, a dose reduction for subsequent courses of therapy is recommended.
Sensory neuropathy occurs frequently with Abraxane. The occurrence of grade 1 or 2 sensory neuropathy does not generally require dose modification. If grade 3 sensory neuropathy develops, treatment should be withheld until resolution to grade 1 or 2 followed by a dose reduction for all subsequent courses of Abraxane.
Because the exposure and toxicity of paclitaxel can be increased with hepatic impairment, administration of Abraxane in patients with hepatic impairment should be performed with caution. The starting dose should be reduced for patients with moderate and severe hepatic impairment.
Injection site reactions occur infrequently with Abraxane and were mild in the randomized clinical trial. Given the possibility of extravasation, it is advisable to closely monitor the infusion site for possible infiltration during drug administration.
It is not known whether paclitaxel is excreted in human milk. Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants, it is recommended that nursing be discontinued when receiving Abraxane therapy.
Adverse events such as fatigue, lethargy, and malaise may affect the ability to drive and use machines.
Campaigners disagreed with the report concerning terminal cancer patient treatment strategy, especially the exclusion of the drugs that were expected to prolong life for terminal cancer patient.
A report on managing cancer costs, made by 37 cancer experts from developed countries, was published in the Lancet Oncology on September 26 . The study highlights the need of a judicious medication for terminal cancer patient. Professor Richard Sullivan has presented the study at the European Multidisciplinary Cancer Congress in Stockholm. Terminal cancer therapy is “futile and potentially inconsistent with patients’ wishes’“, according to the study.
Much of terminal cancer therapy is "futile and potentially inconsistent with patients’ wishes", cancer experts say in Lancet Oncology.
“I would hardly call this type of treatment futile. We have kidney cancer patients on a life-prolonging drug called Sutent who have been told they have only two to three weeks to live but who go on to live for a further five years,” said Rose Woodward, of the James Whale Fund for Kidney Cancer.
“Describing all treatments near the end of life as futile is tantamount to writing patients off. Just because they cannot be “cured” does not mean that we cannot give them valuable treatment, care and support,” said a spokesman for the Rarer Cancers Foundation.
“While cancer care can be expensive, it is unjust to put a cost on the lives of patients, especially when modern treatments can often give them precious time with their loved ones and increase their length and quality of life,” said Ian Beaumont of Bowel Cancer UK.
Some life-extending drugs has shown increased positive results for certain terminal cancer patients.
Abiraterone, for prostate cancer, was approved in the UK at a cost of £35,000 a patient last week. On average it only extends lives by a few weeks, but some patients survive for five years.
Avastin, for advanced bowel cancer, was initially thought to extend survival by an average of only six weeks. Some patients are still alive five years later and with no tumors relapse.
Daily Mail presented the case of Barbara Moss who was given several months to live when she was diagnosed with advanced bowel cancer that had metastasized to her liver in November 2006. She paid for Avastin privately and the drug shrank the tumors and they were small enough to be removed by surgery and she has lived an extra five years.
Zelboraf, a targeted medicine for inoperable or metastatic melanoma BRAF V600E mutation-positive, has shown it increased survival rate of the patients and was approved by FDA last month.
Adcetris, the first drug approved by the FDA for Hodgkin lymphoma in more than 30 years, an antibody-drug conjugate (ADC) directed to CD30, has demonstrated a high durable complete remission rate in CD30-positive malignancies.
Some life-extending drugs has shown increased positive results for certain terminal cancer patients.
Other medicines are still in a trial stage, but some of them are very promising even for terminal cancer.
Scientists from the University of Pennsylvania have genetically engineered patients’ T cells to attack cancer cells in advanced cases of a common type of leukemia. Two of three patients studied have been cancer-free for more than one year. In the third case over 70% of cancer cells were removed.
Researchers from Lund University have identified a method that may attack and destroy prostate cancer stem cells and might lead to a complete cure.
Recently presented data have shown Zybrestat, a pro-drug vascular disrupting agent, helped improve the one-year survival rate of patients with larger anaplastic thyroid cancer tumors.
Specialists at London’s Royal Marsden Hospital have tested radium-223 chloride (a powerful alpha radiation drug for prostate cancer) on 461 patients while another group of the same number was being treated with placebo. The group taking the new drug experienced less pain, side effects and lived longer, and the doctors decided to stop the trial and started treating all 922 patients taking part in the study because they said it would be unethical not to.
Giving a terminal cancer patient false hope is unethically, but in the same time to refuse a potentially helpful treatment to a terminal cancer patient is unethically too. This is not a recent debate, unfortunately health services and terminal cancer still need adjustments, but these can be done by trying and studying.
Roche’s new drug Zelboraf (also known as PLX4032 and vemurafenib) was approved by the FDA on August 17th 2011 for treatment of melanoma patients whose tumors have BRAF mutations (new Zelboraf announcement order). Now that the drug has been approved, your doctor can prescribe it after determining that your tumor has this mutation.
In clinical trials with Zelboraf, patients’ tumors stopped growing for several months and patients were 63% less likely to die during the trial, as compared to those receiving chemotherapy. Be sure to find out if Zelboraf is right for you before you order.
Zelboraf is being approved with a first-of-a-kind test called the cobas 4800 BRAF V600 Mutation Test, a companion diagnostic that will help determine if a patient’s melanoma cells have the BRAF V600E mutation.
The BRAF protein is normally involved in regulating cell growth, but is mutated in about half of the patients with late-stage melanomas. Zelboraf is a BRAF inhibitor that is able to block the function of the V600E-mutated BRAF protein.
“This has been an important year for patients with late-stage melanoma. Zelboraf is the second new cancer drug approved that demonstrates an improvement in overall survival,” said Richard Pazdur, M.D., director of the Office of Oncology Drug Products in the FDA’s Center for Drug Evaluation and Research. “In March, we approved Yervoy (ipilimumab), another new treatment for late-stage melanoma that also showed patients live longer after receiving the drug.”
What to know before you order? Zelboraf’s side effects.
The most common side effects reported in patients receiving Zelboraf included joint pain, rash, hair loss, fatigue, nausea, and skin sensitivity when exposed to the sun. About 26 percent of patients developed a skin-related cancer called cutaneous squamous cell carcinoma, which was managed with surgery. Patients treated with Zelboraf should avoid sun exposure. Patients that develop squamous cell carcinoma as a side effect of Zelboraf are treated by surgery and can continue with treatment
Use of ordered ZELBORAF and Important Side Effect Information for Zelboraf
This information does not take the place of talking to your doctor about your medical condition or your treatment with ZELBORAF.
ZELBORAF is a prescription medicine used to treat a type of skin cancer called melanoma, that has spread to other parts of the body or cannot be removed by surgery, and has a certain type of abnormal “BRAF” gene.
ZELBORAF may cause a type of skin cancer called cutaneous squamous cell carcinoma (cuSCC). CuSCC usually does not spread to other parts of the body. Check your skin and tell your doctor about skin changes including a new wart, a sore or bump that bleeds or does not heal, or a mole that changes size or color.
While taking ZELBORAF, you should avoid going out in the sun. When you go outside, wear clothes that protect your skin, including head, face, hands, arms, and legs. Use lip balm and a broad-spectrum sunscreen with SPF 30 or higher.
Possible serious side effects of ZELBORAF include severe allergic reactions, severe skin reactions, changes in the electrical activity of your heart called QT prolongation, which can potentially be life-threatening, abnormal liver function tests, eye problems, or new melanoma lesions.
Common side effects of ZELBORAF include joint pain, rash, hair loss, tiredness, sunburn or sun sensitivity, nausea, itching, or warts. You need to know these before ordering Zelboraf.
These are not all of the possible side effects of ZELBORAF. Tell your doctor if you have any side effect that bothers you or does not go away. For more information about side effects, ask your doctor or pharmacist.
Call your doctor for medical advice about any side effects. You may report side effects to the FDA at 1-800-FDA-1088. You may also report side effects to Genentech at 1-888-835-2555.
With Zelboraf’s approval, your doctor can now prescribe this drug for you if your tumor has the BRAF mutation. To test the tumor, your doctor would order a laboratory test.
Several clinical trials are testing whether a combination of Zelboraf with other drugs might work better than Zelboraf alone. One exciting clinical trial combines Zelboraf with Yervoy, a new immunotherapy drug (Order more details about Zelboraf clinical trials). The following table lists some of these clinical trials that Zelboraf went through, and by clicking on the name of a trial you can learn more about the drug used and the types of patients that the trial is looking for.
Zelboraf Summary for Ordered Clinical Trials
Name(s)
Target
Manufacturer
Status
Zelboraf, PLX4032, vemurafenib, RO5185426, RG7204
BRAF
Hoffmann-La Roche
Approved for melanoma patients with BRAF mutations
In July 2011, the FDA issued a new draft guidance to facilitate the development and review of companion diagnostics. The guidance, currently available for public comment, is intended to provide companies with guidance on the agency’s policy for reviewing a companion diagnostic and the corresponding drug therapy.
Relevant Links for More Information on Zelboraf Ordering
Melanoma is the leading cause of death from skin disease. The National Cancer Institute estimated that 68,130 new cases of melanoma were diagnosed in the United States during 2010; about 8,700 people died from the disease.
Zelboraf is marketed by South San Francisco based-Genentech, a member of the Roche Group. The cobas 4800 BRAF V600 Mutation Test is manufactured by Roche Molecular Systems in Pleasanton, Calif.
Seattle Genetics, Inc. (Nasdaq: SGEN) announced that the U.S. Food and Drug Administration (FDA) has granted accelerated approval of Adcetris (brentuximab vedotin) for two indications.
1. the treatment of patients with Hodgkin lymphoma after failure of autologous stem cell transplant (ASCT) or after failure of at least two prior multi-agent chemotherapy regimens in patients who are not ASCT candidates, and
2. the treatment of patients with systemic anaplastic large cell lymphoma (ALCL) after failure of at least one prior multi-agent chemotherapy regimen.
[googlead tip=”lista_mare” aliniat=”stanga”]The indications for Adcetris are based on response rate. There are no data available demonstrating improvement in patient-reported outcomes or survival with Adcetris.
Adcetris is the first drug approved by the FDA for Hodgkin lymphoma in more than 30 years, and provides a new therapeutic alternative for Hodgkin lymphoma and systemic ALCL in these settings.
Adcetris will be available to patients this week
Seattle Genetics expects to make Adcetris available to patients this week.
Adcetris is an antibody-drug conjugate (ADC) directed to CD30.
“Bringing a new product to the market is a significant milestone for Seattle Genetics in fulfilling its mission to improve the lives of people with cancer,” said Clay B. Siegall, Ph.D., President and Chief Executive Officer of Seattle Genetics.[googlead tip=”vertical_mediu” aliniat=”dreapta”]
“The approval of Adcetris is a result of more than a decade of research and development by talented scientists and physicians. The company has deep appreciation for the hundreds of patients who participated in Adcetris trials, and the passion and determination of the clinicians at sites around the world in investigating this first in a new class of targeted anticancer agents.We are committed to continued clinical investigation of Adcetris through a broad developmentprogram for CD30-positive malignancies, including confirmatory trials in front-line Hodgkin and T-cell lymphomas that we have planned in consultation with the FDA.”
“The marked single agent activity seen with Adcetris, including a high durable complete remission rate, offers an opportunity to improve the treatment paradigm of patients for whom the treatment is indicated,” said Owen A. O’Connor, M.D., Ph.D., Professor, and Director, Division of Hematology and Medical Oncology at NYU Cancer Institute.
“This approval represents a major advancement in the care of these patients.”
Seattle Genetics also announced that it has established a patient assistance program named SeaGenSecure™ that offers patients and providers access to Adcetris reimbursement support, benefit investigations and patient assistance programs.
Seattle Genetics is jointly developing Adcetris with Millennium: The Takeda Oncology Company.
Under the terms of the collaboration agreement, Seattle Genetics has U.S. and Canadian commercialization rights and the Takeda Group has rights to commercialize Adcetris in the rest of the world. Seattle Genetics and the Takeda Group are funding joint development costs for Adcetris on a 50:50 basis, except in Japan, where the Takeda Group will be solely responsible for development costs.
Medical scientists have found a new form of mechanism leading to hereditary cancer susceptibility, demonstrating that minor changes in certain anti-cancer genes might work as magnets to draw altering “biochemical tags”.
The tags successfully switch these genes off as well as predispose families to a higher risk associated with the condition. The researchers, from the University of New South Wales (UNSW), consider that a minor spelling error affecting just one letter in the DNA sequence close to the beginning of the gene is actually what draws in the biochemical marking, named methylation. This methylation switches genes off, thus has specific influences on the DNA.
“Methylation sits on top of our DNA, and provides the instructions to turn the gene off,” pointed out Dr Megan Hitchins.
In one well studied cause of hereditary cancer, alterations in the cancer-prevention gene MLH1 are transferred from mother or father to children. This situation generates up to 80 percent risk of developing bowel cancer, uterine cancer and other malignancies.
On the other hand, a number of family members with hereditary cancer do not have spelling mistakes in MLH1, but alternatively possess methylation placed on the gene.
“When the methylation attaches to the MLH1 gene in these families, it causes it to be completely switched off and as a consequence cancer develops,” affirmed head of the adult cancer program at the Lowy Cancer Research Centre, Professor Robyn Ward. “But until now, we did not understand how these methylation tags were being passed from parent to child.”
Hereditary cancer study: certain anti-cancer genes act like a magnet for methylation that disappears in semen or ova and reappears in child
In the study the researchers investigated three generations of a large family, who had experienced cancer at young age, but in whom no spelling mistakes characteristic for this kind of inherited cancer syndrome had been identified. Noticeably a number of family members from all generations had methylation tags on their gene.
“In this family, biochemical tags attached to the MLH1 gene were present in all three generations. This was intriguing since these markers are usually removed during the production of eggs and sperm. What we found was that a subtle change near the gene was acting like a magnet to attract methylation. So it was not the methylation itself that was being passed from parent to child, but rather the DNA change, and this acted as a methyl magnet,” Dr Megan Hitchins said.
The methylation had disappeared in the semen and ova and after that regenerated in every brand-new generation, the researchers explained.
Professor Robyn Ward said the study had specified the trigger of cancer in this family and it had provided new options for genetic diagnosis, counselling as well as early treatment in other families vulnerable to hereditary cancer.
The group is additionally studying the utilization of specific medications (Epigenetic Reversal Drugs) to remove the methylation in cancer, thus to switch the anti-cancer genes back on again. Later on these medicines might be administered in order to create a more specific method of cancer therapy and perhaps prevention.
Additional scientists linked to this research have been the Genetic Services of Western Australia and School of Paediatrics and Child Health, University of Western Australia.
The study on hereditary cancer was published in the primary international journal “Cancer Cell”.
This website has updated its privacy policy in compliance with EU GDPR 2016/679. Please read this to review the updates about which personal data we collect on our site. By continuing to use this site, you are agreeing to our updated policy. AcceptRejectRead More
Privacy & Cookies Policy
Privacy Overview
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Any cookies that may not be particularly necessary for the website to function and is used specifically to collect user personal data via analytics, ads, other embedded contents are termed as non-necessary cookies. It is mandatory to procure user consent prior to running these cookies on your website.